Clinical31 October 2025 ProDental Partners with The Royal College of Surgeons of Edinburgh (RCSEd)Posted by KathySHARE
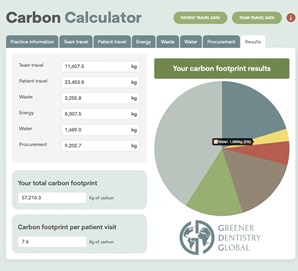
Clinical9 September 2024 From Classrooms to Clinics: Calculating a Sustainable Future in DentistryPosted by GemmaSHARE